
You’re offline. This is a read only version of the page.

If you have concerns about following these guidelines please consult your A&E senior or the Orthopaedic Registrar on-call.
Please refer to the correct team as below
For Adult Virtual Fracture Clinic:
Please use the online referral form
We are an acute service and only manage injuries within the first 6 weeks
All patients referred to the Adult Virtual Fracture Clinic require x-rays except calf muscle tears and suspected Achilles tendon injuries
Please put as much information about the patient on the referral as possible
This team can be contacted by email on uhsussex.fracturecare@nhs.net or via ext 63428
Minor soft tissue injuries do not routinely require a VFC referral and usually resolve with time. Patients can self-refer to MSK Partnership if their symptoms do not resolve within 6 weeks.
Please note- we DO NOT accept referrals for:
If the referral does not fit our criteria it may be declined and returned to you via email
For Virtual Hand and Wrist Fracture Clinic:
For the Paediatric Virtual Fracture Clinic:
Click below to jump to body region:
|
Spine |
|---|
|
Fracture |
Subcategory |
A&E Management |
| C-spine fracture | Refer to spinal on-call during the day, neurosurgery during the night | |
| L-spine fracture | Stable wedge fracture | Refer to spinal on-call during the day, neurosurgery during the night |
| All others | Refer to spinal on-call during the day, neurosurgery during the night | |
| T-spine fracture | Refer to spinal on-call during the day, neurosurgery during the night | |
| Spine sprains/whiplash injuries | Please do not refer to virtual fracture clinic, GP refer into MSK service if necessary | |
| Non-traumatic neck/back pain |
Exclude infection Do not refer to virtual fracture clinic GP review or refer to spine service as outpatient |
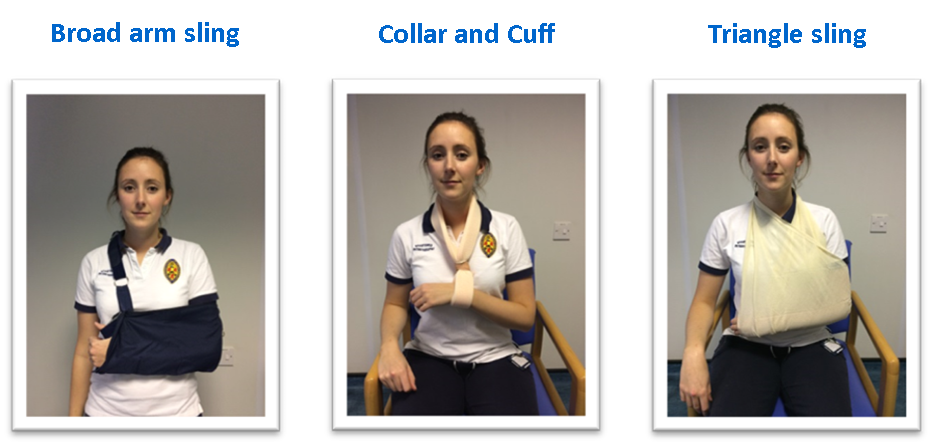
Types of slings:
|
Fracture |
Subcategory |
A&E Management |
|
| Sternoclavicular joint dislocation | Anterior or superior |
Polysling Analgesia On-line referral to virtual fracture clinic |
|
| Posterior | Refer to Ortho on-call team | ||
| Clavicle fractures | Open fracture, threat to skin and/or neurovascular compromise |
Refer to Ortho on-call team |
|
| Closed injury, no threat to skin or neurovascular compromise |
Polysling/double collar and cuff Analgesia On-line referral to virtual fracture clinic |
||
| Acromioclavicular joint injuries | Closed, neurovascular intact and skin not under threat |
Polysling/double collar and cuff Analgesia On-line referral to virtual fracture clinic |
|
| Any evidence of open injury, neurovascular compromise or threat to skin |
Refer to ortho reg on call |
||
| Soft tissue shoulder injuries | Acute on chronic |
Polysling or double loop collar & cuff Analgesia Contact GP or self-refer to MSK partnership if not settling with 6 weeks |
|
| Acute Minor soft tissue injuries |
Polysling or double loop collar & cuff Analgesia Contact GP or self-refer to MSK partnership if not settling with 6 weeks |
||
| Suspected rotator cuff tears and long head of biceps tendon ruptures |
Polysling or double loop collar & cuff Analgesia On-line referral to virtual fracture clinic |
||
| Anterior Shoulder Dislocations | Primary Dislocation |
Reduce Polysling Analgesia On-line referral to virtual fracture clinic |
|
| Recurrent Dislocation |
Reduce Polysling Analgesia On-line referral to virtual fracture clinic |
||
|
Shoulder fracture dislocation Post reduction |
Non-displaced fracture |
Polysling Analgesia On-line referral to virtual fracture clinic |
|
| Displaced fracture |
Refer to Ortho on-call |
||
| Posterior shoulder dislocations | Traumatic or following epileptic seizure |
Refer to Ortho on-call for advice before reduction. A proximal humeral fracture must be excluded. |
|
| Previous multiple posterior dislocations (normally due to multidirectional instability) |
Reduce Polysling Analgesia On-line referral to virtual fracture clinic |
||
|
Acute Atraumatic Shoulder Pain (including Calcific Tendonitis) |
Exclude infection (temp, FBC, CRP) and other red flags. Collar & Cuff (single or double loop) Analgesia Refer to GP |
||
|
Proximal humeral fractures |
Minimally displaced greater tuberosity and or surgical neck fracture |
Collar & Cuff Analgesia On-line referral to virtual fracture clinic |
|
|
Displaced fracture or more than 2 part fracture (providing neurovascularly intact) |
Collar & cuff Online referral to VFC |
||
|
If any concerns re: neurovascular status |
Ortho reg on call |
||
|
Humeral shaft fractures |
Open fracture, significantly displaced or radial nerve injury |
Refer to Ortho on-call |
|
|
Closed fracture, reasonable alignment & radial nerve intact |
Collar & Cuff Analgesia On-line referral to virtual fracture clinic |
||
|
Distal Biceps tendon rupture |
Refer to Ortho on-call |
||
|
Distal humeral fracture |
Refer to Ortho on-call |
||
|
Olecranon fractures |
Undisplaced |
Above elbow backslab Collar and Cuff Analgesia On-line referral to virtual fracture clinic |
|
|
Displaced |
Refer Ortho on-call |
||
|
Radial head/neck fractures Occult proximal radius fractures |
Radiohumeral joint located & no associated fracture of ulna |
Collar & cuff (single or double loop) or polysling Analgesia Online referral to virtual fracture clinic and give patient care plan for proximal radius fracture or occult proximal radius fracture and advise will only be contacted if a change in management is required |
|
|
Radiohumeral joint subluxed or dislocated and/or associated fracture of ulna |
Refer Ortho on-call |
||
|
Dislocated elbow |
Relocate under sedation Polysling - elbow in 90 degrees flexion Analgesia On-line referral to virtual fracture clinic |
||
|
Fracture dislocation elbow Post reduction |
Refer to ortho reg |
||
|
Radial & ulna midshaft fractures Any fractures within 5cm of wrist should be referred to VHFC. |
Nightstick ulna (undisplaced) |
Above elbow cast (90deg flexion, neutral rotation) Polysling Analgesia On-line referral to virtual fracture clinic |
|
|
All others |
Refer Ortho on-call |
||
|
Fracture |
Subcategory |
A&E Management |
|
| Pelvic fracture | APC, LC, VS |
Treat hypovolaemia Refer Ortho on-call |
|
| Low energy, elderly pubic rami fractures | Mobilise FWB, investigate cause of fall, discharge planning as per best practise tariff | ||
| Avulsion fractures | Refer Ortho on-call | ||
| Acetabular fracture | Refer Ortho on-call | ||
| Neck of femur | Refer Ortho on-call | ||
| Dislocated Total hip replacement | First dislocation |
Refer Ortho on-call For reduction in theatre |
|
| Had previous dislocation |
Reduce in ED if possible or refer Ortho on-call Even if reduced and patient fit for discharge please give details to Ortho Reg on-call to make out-patient appointment with relevant consultant |
||
| Hip pain post fall, no fracture on plain x-ray | If able to fully weight bear |
Discharge If ongoing issues to reattend ED or see GP |
|
| Unable to FWB |
Further imaging to exclude fracture If no fracture discharge |
||
| Femoral shaft fracture | Refer Ortho on-call | ||
| Distal femoral fracture | Refer Ortho on-call | ||
| Thigh injury/haematoma | Exclude compartment syndrome | Discharge | |
| Proximal hamstring tendon rupture | Refer Ortho on-call | ||
| Calf Muscle Tear |
Ensure Achilles tendon injury is ruled out by Simmonds testing and palpation If any doubt about Achilles treat as suspected Achilles rupture |
Weight bear as tolerated Boot +/- 3 wedges for comfort if required. Advised to wean off wedges as soon as able. If significant injury, refer to VFC. |
|
| Acute soft tissue knee injuries (within last 6 weeks) |
Mild soft tissue knee injury |
Reassure likely to resolve with time Mobilise FWB and encourage ROM See GP 6/52 if still symptomatic |
|
|
Acute on chronic OA exacerbation |
Discharge to GP Advise to self-refer to MSK Partnership if doesn’t settle |
||
| Patella tendon rupture or quads tendon rupture |
Refer Ortho on-call |
||
| Suspected acute meniscal tear or ligament injury without true locking/block to extension |
Crutches to aid mobility if required Complete VTE Risk Assessment if CPS given X-rays and online referral to virtual fracture clinic |
||
| Suspected acute meniscal tear with true locking/block to extension |
Refer to Ortho on-call as locked knee |
||
| Atraumatic painful/swollen knee | Apyrexial, normal CRP & WCC. No infection or other red flags. | Discharge back to GP | |
| Any of the above infectious signs/red flags or recent knee surgery | Refer to Ortho on-call | ||
|
Patella Fracture |
Un-displaced |
Cricket pad splint Full weight bearing Online referral to virtual fracture clinic |
|
| Displaced or vulnerable to displacement |
Refer to Ortho on-call |
||
|
Patella dislocation |
Primary |
Reduce AP, Lateral & Skyline x-ray Cricket pad splint Full WB, crutches if needed On-line referral to virtual fracture clinic |
|
| Recurrent |
Reduce AP, Lateral & Skyline x-ray Cricket pad splint if needed Full WB On-line referral to virtual fracture clinic |
||
|
Tibial plateau fractures |
Refer Ortho on-call Above knee backslab VFC will decline any referral for a tibial plateau fracture |
||
|
Tibia |
Proximal |
Refer Ortho on-call Above knee backslab |
|
| Shaft: undisplaced |
Refer Ortho on-call Above knee backslab |
||
| Shaft: displaced |
Refer Ortho on-call Reduce & above knee backslab |
||
| Distal/Pilon fractures |
Refer Ortho on-call |
||
| Proximal and Mid-shaft fibula fractures | Proximal fibula fracture |
Screen for ankle pain/possible maisonneuve injury. If positive, refer to Ortho on-call. If negative: Weight bear as tolerated Online referral to virtual fracture clinic |
|
| Mid-shaft fibula fracture |
Screen for ankle pain/possible maisonneuve injury. If positive, refer to Ortho on-call. WB ankle views (if possible) If negative: Boot for comfort (optional)- if given complete VTE Risk Assessment Crutches Weight bear as tolerated Online referral to virtual fracture clinic |
||
| Soft tissue ankle injury/sprain |
Compression bandage Black boot if severe- Complete VTE Risk Assessment Weight bear as tolerated Most soft tissue ankle injuries do not need referral to VFC. Refer only if severe injury or clinical concerns. |
||
|
Ankle fractures |
Weber A fibula fracture |
Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
|
|
Weber B fibula fracture No talar shift |
Black boot Weight bear as tolerated On-line referral to virtual fracture |
||
|
Weber B fibula fracture Talar shift |
If concern re: talar shift then complete weight bearing ankle XRs (mortise and lateral) or CT scan and discuss with ortho on call | ||
|
Weber C No talar shift |
Black boot Refer Ortho on-call |
||
|
Weber C Talar shift |
Reduce Backslab Refer Ortho on-call |
||
| Posterior mallelous fracture (isolated) |
Black boot (non-weight bearing) Refer Ortho on-call |
||
| Bimalleolar/trimalleolar |
Reduce if needed Backslab and CT scan Refer Ortho on-call |
||
| Medial Malleolus fractures |
Isolated medial malleolus Small Fragment- undisplaced |
X-Ray of full length tibia/fibula must be done to rule out proximal fibula fracture. If fracture identified, refer to ortho on call. Weight bearing ankle x-rays (if possible) If no proximal fibula fracture: Black boot Weight bear as tolerated. On-line referral to virtual fracture clinic |
|
|
Isolated medial malleolus Large fragment - undisplaced |
Refer Ortho on-call |
||
|
Isolated medial malleolus Displaced |
Refer Ortho on-call |
||
| Hindfoot injuries | Talus or Calcaneal fractures +/- dislocation |
CT Backslab Refer Ortho on-call |
|
| Small avulsion fractures of calcaneum |
Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
||
| Avulsion fracture from talus |
Black boot On-line referral to virtual fracture clinic |
||
| Achilles tendon rupture |
If diagnosis in doubt consult A&E senior or Ortho Registar on-call Rebound boot with 5 wedges or, if unavailable, black boot with 5 wedges. Urgent outpatient USS to be requested Weight bear as tolerated. Prophylactic Enoxaparin prescribed for 42 days Please print this advice leaflet and give to patient Online referral to virtual fracture clinic |
||
| Midfoot injuries | Avulsion fractures of tarsal bones |
Black boot Full weight bear Online referral to virtual fracture clinic |
|
|
Tarsal fractures - Undisplaced (Navicular, cuboid, cuneiforms) |
Black boot NWB On-line referral to virtual fracture clinic |
||
| Tarsal fractures - Displaced |
Backslab CT Refer Ortho on-call |
||
|
Lis-franc fracture / dislocation Including suspected on basis of mechanism / swelling / planter bruising |
CT Backslab Refer Ortho on-call |
||
|
Metatarsal fractures |
Base of metatarsal fractures- undisplaced |
CT scan for VFC review Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
|
| Base of metatarsal fractures- displaced |
CT Blackboot NWB Refer Ortho on-call |
||
| 1st metatarsal fracture |
Black boot Heel weight bear On-line referral to virtual fracture clinic |
||
| 2nd-4th metatarsal - single fracture |
Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
||
| 2nd-4th metatarsal - multiple fractures |
Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
||
| Midshaft of 5th metatarsal fracture |
Black boot Weight bear as tolerated On-line referral to virtual fracture clinic |
||
| Base of 5th metatarsal fracture |
Black boot three weeks Weight bear as tolerated Give patient care plan and advise will only be contacted if a change in management is required Online referral to virtual fracture clinic and give patient care plan and advise will only be contacted if a change in management is required |
||
| Toe fractures | Hallux phalanx fracture - intra-articular |
Black boot/loose shoe If boot given- Complete VTE Risk Assessment Weight bear as tolerated Online referral to virtual fracture clinic and give patient care plan and advise will only be contacted if a change in management is required If there is a wound, to be followed up by GP Practice nurse |
|
| Hallux Phalanx fracture - undisplaced |
Black boot for up to three weeks/loose shoe Weight bear as tolerated Discharge |
||
| Hallux Phalanx fracture - displaced |
Reduce Black boot/loose shoe Weight bear as tolerated Online referral to virtual fracture clinic and give patient care plan and advise will only be contacted if a change in management is required If there is a wound, to be followed up by GP Practice nurse |
||
| Lesser phalanx fracture |
Neighbour strap two weeks Weight bear as tolerated Discharge |
||
| Toe dislocations |
Reduce Neighbour strap two weeks Weight bear as tolerated Discharge unless reduction is unstable. If unstable, online referral to virtual fracture clinic. |
||